Care Pathways: Familial Adenomatous Polyposis
HEREDITARY
5/7/20241 min read
Care Pathways: Familial Adenomatous Polyposis
Patients with familial adenomatous polyposis (FAP) present in many different ways and their phenotype included multiple neoplasms in many different organs. The Care pathways for affected patients must be flexible, and able to account for differences in presentation and the context of the patient.
Although FAP is an autosomal dominantly inherited condition with almost 100% penetrance, 25% pf patients do not have a family history. This may be because of active concealment of the disease by parents, ignorance of the parents, non-paternity, maternal mosaicism, or most likely, a de novo mutation. The bottom line is that these patients have no idea of their risk and present late, with symptoms.
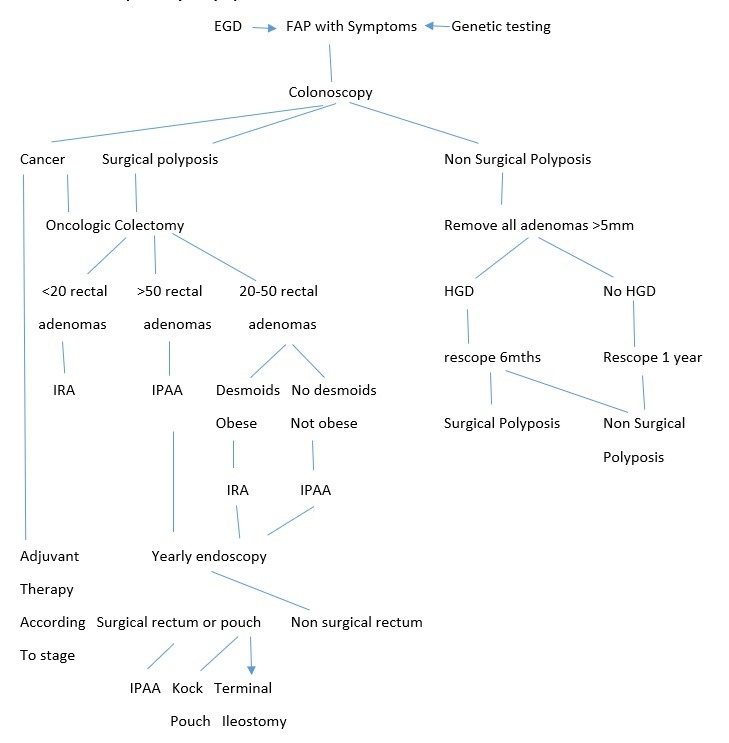
Colorectal Care pathway 1: Symptoms
Surgical polyposis:
1. Obvious cancer 2. Endoscopically suspicious lesions 3. PV APC 1309 4. Polyposis not controllable endoscopically 5. >10 large (>10mm) adenomas 6. Rapid increase in polyp numbers 7. Symptomatic polyposis 8. Multiple lesions with high grade dysplasia
Non surgical polyposis:
1. Endoscopically treatable polyps 2. Polyps <5mm with <10 polyps >10mm 3. Stable polyp counts ± 50 polyps 4. Attenuated polyposis (<100) 5. High risk of desmoids 6. No high grade dysplasia
Colorectal Care pathway 2: Genotype
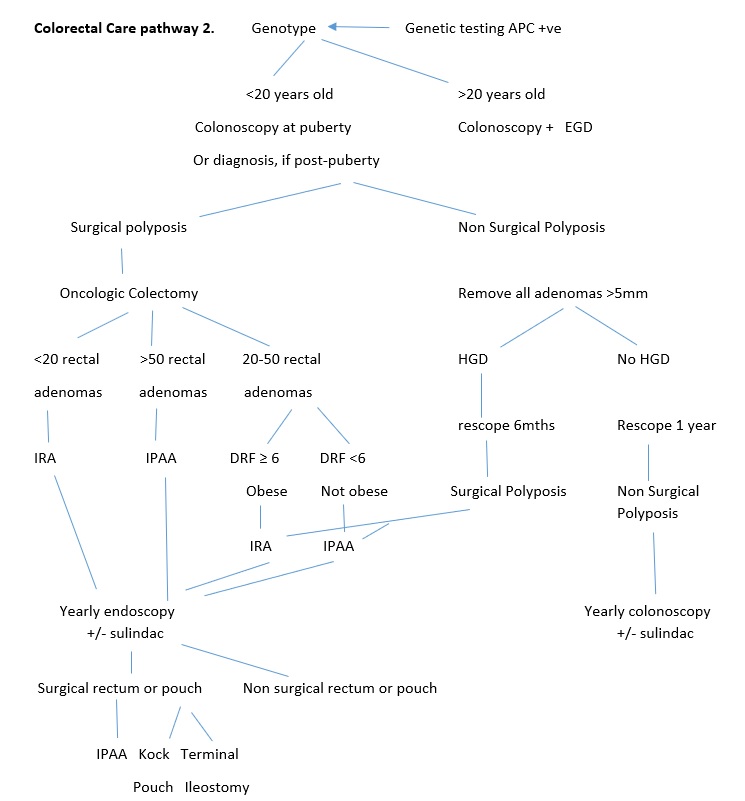

Surgical polyposis:
1. Obvious cancer 2. Endoscopically suspicious lesions 3. PV APC 1309 4. Polyposis not controllable endoscopically 5. >10 large (>10mm) adenomas 6. Rapid increase in polyp numbers 7. Symptomatic polyposis 8. Multiple lesions with high grade dysplasia
Non surgical polyposis:
1. Endoscopically treatable polyps 2. Polyps <5mm with <10 polyps >10mm 3. Stable polyp counts ± 50 polyps 4. Attenuated polyposis (<100) 5. High risk of desmoids 6. No high grade dysplasia
DRF = desmoid risk factor